
Abstract
Objective
The main goal of the current study was to compare survival differences among subgroups of primary ovarian cancer patients in International Federation of Gynecology and Obstetrics (FIGO) stages IIIC and IIIA1 after complete tumor debulking surgery.
Methods
A total of 218 patients with primary ovarian cancer who received complete cytoreductive surgery were included in the current retrospective analysis of the validated Tumor Bank Ovarian Cancer Network Database, which covers the periods January 2002 until December 2012. According to their tumor spread pattern, patients were divided into three groups: Group A (peritoneum only), Group B (peritoneum and lymph nodes), and Group C (lymph nodes only). Associations between groups and clinicopathological factors were analyzed using standard statistical procedures.
Results
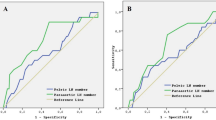
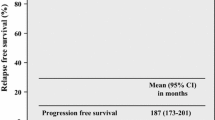
The vast majority of patients were classified into Group B. Lymph node involvement was detected in 70.5 % of the cases where peritoneal implants presented ≥2 cm beyond the pelvis (Group A + B). The estimated 5-year overall survival (OS) rates were 47.4 % in Group A, 45.1 % in Group B, and 91.7 % in Group C (p < 0.01). In the subgroup analysis of Group B, both pelvic and para-aortic lymph node involvement was found in 57 % of patients. Patients in Group B who had para-aortic lymph node involvement only had better median progression-free survival (PFS) compared with patients with pelvic lymph node involvement only and pelvic and para-aortic lymph node involvement (28, 16, and 18 months, respectively; p = 0.02). The median OS differed significantly between patients with para-aortic lymph node involvement only versus patients with both pelvic and para-aortic involvement (68.5 vs. 46.7 months; p = 0.02). Three-year PFS was 90.0 % in FIGO IIIA1(i) and 62.6 % in FIGO IIIA1(ii) (hazard ratio 2.30, 95 % confidence interval 0.45–11.58).
Conclusions
Patients with FIGO stage IIIC with lymph node involvement only had the best clinical outcome compared with patients in the same stage with peritoneal involvement only. Furthermore, involvement of both pelvic and para-aortic lymph nodes were of the same infrequency, and involvement of only para-aortic lymph nodes in this stage resulted in a better chance of survival than involvement of pelvic lymph nodes only or both pelvic and para-aortic lymph nodes simultaneously. In accordance with the revised FIGO classification of 2013, our study revealed that FIGO IIIA1(i) is prognostically better compared with FIGO IIIA1(ii).


Similar content being viewed by others

References
Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90.
Pickel H, Lahousen M, Stettner H, et al. The spread of ovarian cancer. Baillières Clin Obstet Gynaecol. 1989;3(1):3–12.
Burghardt E, Girardi F, Lahousen M, et al. Patterns of pelvic and paraaortic lymph node involvement in ovarian cancer. Gynecol Oncol. 1991;40(2):103–6.
Heintz APM, Odicino F, Maisonneuve P, et al. Carcinoma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet. 2006;95 Suppl 1:S161–92.
Engel J, Eckel R, Schubert-Fritschle G, et al. Moderate progress for ovarian cancer in the last 20 years: prolongation of survival, but no improvement in the cure rate. Eur J Cancer. 2002;38(18):2435–45.
Nguyen HN, Averette HE, Hoskins W, et al. National survey of ovarian carcinoma. VI. Critical assessment of current International Federation of Gynecology and Obstetrics staging system. Cancer. 1993;72(10):3007–11.
Jemal A, Tiwari RC, Murray T, et al. Cancer statistics, 2004. CA Cancer J Clin. 2004;54(1):8–29.
Meyers MA. Distribution of intra-abdominal malignant seeding: dependency on dynamics of flow of ascitic fluid. Am J Roentgenol Radium Ther Nucl Med. 1973;119(1):198–206.
Spirtos NM, Gross GM, Freddo JL, et al. Cytoreductive surgery in advanced epithelial cancer of the ovary: the impact of aortic and pelvic lymphadenectomy. Gynecol Oncol. 1995;56(3):345–52.
Di Re F, Baiocchi G, Fontanelli R, et al. Systematic pelvic and paraaortic lymphadenectomy for advanced ovarian cancer: prognostic significance of node metastases. Gynecol Oncol. 1996;62(3):360–5.
Sakai K, Kamura T, Hirakawa T, et al. Relationship between pelvic lymph node involvement and other disease sites in patients with ovarian cancer. Gynecol Oncol. 1997;65(1):164–8.
Onda T, Yoshikawa H, Yokota H, et al. Assessment of metastases to aortic and pelvic lymph nodes in epithelial ovarian carcinoma. A proposal for essential sites for lymph node biopsy. Cancer. 1996;78(4):803–8.
Shimizu Y. Validity of complete paraaortic and pelvic lymphadenectomy in apparent stage I (T1) epithelial ovarian carcinoma [in Japanese]. Nihon Rinsho. 2004;62 Suppl 10:570–7
Prat J, FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int J Gynaecol Obstet. 2014;124(1):1–5.
Trimbos JB, Vergote I, Bolis G, et al. Impact of adjuvant chemotherapy and surgical staging in early-stage ovarian carcinoma: European Organisation for Research and Treatment of Cancer–Adjuvant Chemotherapy in Ovarian Neoplasm Trial. J Natl Cancer Inst. 2003;95(2):113–25.
Zanetta G, Rota S, Chiari S, et al. The accuracy of staging: an important prognostic determinator in stage I ovarian carcinoma. A multivariate analysis. Ann Oncol. 1998;9(10):1097–101.
Onda T, Yoshikawa H, Yasugi T, et al. Patients with ovarian carcinoma upstaged to stage III after systematic lymphadenctomy have similar survival to stage I/II patients and superior survival to other stage III patients. Cancer. 1998;83(8):1555–60.
Baek S-J, Park J-Y, Kim D-Y, et al. Stage IIIC epithelial ovarian cancer classified solely by lymph node metastasis has a more favorable prognosis than other types of stage IIIC epithelial ovarian cancer. J Gynecol Oncol. 2008;19(4):223–8.
Delgado G, Oram DH, Petrilli ES. Stage III epithelial ovarian cancer: the role of maximal surgical reduction. Gynecol Oncol. 1984;18(3):293–8.
Griffiths CT, Parker LM, Fuller AF Jr. Role of cytoreductive surgical treatment in the management of advanced ovarian cancer. Cancer Treat Rep. 1979;63(2):235–40.
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47.
Cliby WA, Aletti GD, Wilson TO, et al. Is it justified to classify patients to Stage IIIC epithelial ovarian cancer based on nodal involvement only? Gynecol Oncol. 2006;103(3):797–801.
Berek JS. Lymph node-positive stage IIIC ovarian cancer: a separate entity? Int J Gynecol Cancer. 2009;19 Suppl 2:S18–20.
Carnino F, Fuda G, Ciccone G, et al. Significance of lymph node sampling in epithelial carcinoma of the ovary. Gynecol Oncol. 1997;65(3):467–72.
Grossi E, Noli S, Scarfone G, et al. Ten years survival of FIGO stage IIIC epithelial ovarian cancer cases due to lymph node metastases only. Eur J Gynaecol Oncol. 2012;33(6):615–6.
Morice P, Joulie F, Camatte S, et al. Lymph node involvement in epithelial ovarian cancer: analysis of 276 pelvic and paraaortic lymphadenectomies and surgical implications. J Am Coll Surg. 2003;197(2):198–205.
Ayhan A, Gultekin M, Taskiran C, Celik NY, Usubutun A, Kucukali T, et al. Lymphatic metastasis in epithelial ovarian carcinoma with respect to clinicopathological variables. Gynecol Oncol. 2005;97(2):400–4.
Ayhan A, Gultekin M, Dursun P, et al. Metastatic lymph node number in epithelial ovarian carcinoma: does it have any clinical significance? Gynecol Oncol. 2008;108(2):428–32.
Panici PB, Maggioni A, Hacker N, et al. Systematic aortic and pelvic lymphadenectomy versus resection of bulky nodes only in optimally debulked advanced ovarian cancer: a randomized clinical trial. J Natl Cancer Inst. 2005;97(8):560–6.
Maggioni A, Benedetti Panici P, Dell’Anna T, et al. Randomised study of systematic lymphadenectomy in patients with epithelial ovarian cancer macroscopically confined to the pelvis. Br J Cancer. 2006;95(6):699–704.
Burghardt E, Lahousen M, Stettner H. The significance of pelvic and para-aortic lymphadenectomy in the operative treatment of ovarian cancer. Baillières Clin Obstet Gynaecol. 1989;3(1):157–65.
Chambers SK. Systematic lymphadenectomy in advanced epithelial ovarian cancer: two decades of uncertainty resolved. J Natl Cancer Inst. 2005;97(8):548–9.
Parazzini F, Valsecchi G, Bolis G, et al. Pelvic and paraortic lymph nodal status in advanced ovarian cancer and survival. Gynecol Oncol. 1999;74(1):7–11.
Acknowledgment
This Project was supported by a research Grant from Berliner Krebsgesellschaft e.V.
Author information
Authors and Affiliations
Corresponding author
Additional information
FIGO IIIC: according to the FIGO classification of 1985.
FIGO IIIA1: according to the revised FIGO classification of 2013.
Rights and permissions
About this article

Cite this article
Gasimli, K., Braicu, E.I., Nassir, M. et al. Lymph Node Involvement Pattern and Survival Differences of FIGO IIIC and FIGO IIIA1 Ovarian Cancer Patients After Primary Complete Tumor Debulking Surgery: A 10-Year Retrospective Analysis of the Tumor Bank Ovarian Cancer Network. Ann Surg Oncol 23, 1279–1286 (2016). https://doi.org/10.1245/s10434-015-4959-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4959-4